


 Research Article
Research Article
Knowledge About Cervical Cancer Among Urban and Rural Women in The East Coast of Malaysia
Received Date:September 28, 2022; Published Date:November 17, 2022
Abstract
Cervical cancer is the third leading cause of death among at-risk reproductive women in Malaysia. This study was to find out the level of knowledge about cervical cancer among urban and rural women. The study involved women aged between 30 and 65 years. The design of this comparative study was conducted to compare the level of cervical cancer knowledge among urban and rural women. The sampling method uses a probability sampling method based on sampling criteria and sample exclusion criteria. The IBM Corp.’s 2013 Statistical Package for Social Sciences (SPSS) version 20 software was used to analyse the data in this study. The results show that the percentage of this knowledge is good for urban and rural women on the east coast of Malaysia..
Keywords:Knowledge; Cervical Cancer; Urban; Rural Women
Introduction
Cervical cancer is a major public health problem. In 2019, cervical cancer is the third leading cause of death (7.7%) among women in Malaysia [1]. In Australia, by 2020 it is estimated that less than 4 new cases per year from 100,000 women will develop cervical cancer and less than 6 new cases per year from 100,000 women by 2028 if attitudes toward periodic screening practices are improved [2]. The level of knowledge about cervical cancer among urban and rural women in Terengganu was measured to identify the population of having knowledge about it. The study involved women aged between 30 and 65 years. The design of this comparative study was conducted to compare the level of cervical cancer knowledge among urban and rural women. The results show that the percentage of this knowledge is still low for urban and rural women on the east coast of Malaysia.
Literature Review
Cervical cancer is defined as cancer that originates from the cervix. Cervical cancer is the presence of HPV caused by a sexually transmitted viral infection. If no treatment is given, it will spread to cancer. Cervical cancer is one of the leading causes of death in developing countries. About 80% of sexually active American women have been infected with HPV. Men are also carriers of HPV. However, not all types of HPV cause cancer, only 12 types of viruses that are at high risk of causing cancer and two types of viruses (HPV 16 & HPV 18) are responsible for 70% of cervical cancer. This abnormal cell growth will invade or spread to other parts. It usually occurs without symptoms. Further symptoms can be seen through abnormal vaginal bleeding, pelvis pain or pain during sexual intercourse [3].
The results of the study of Endalew et al. [4], showed that only 26.2% of respondents were knowledgeable about cervical cancer screening. The majority of respondents (83.8%) had heard of cervical cancer. But about 76.9% of respondents are unaware of the symptoms of cervical cancer. While 8.8%, 5.0%, 5.0%, and 0.4%of respondents believed that having multiple sexual partners, onset of sexual intercourse at a young age, smoking, and HPV infection were major risk factors for cervical cancer. In fact, 97.7% of respondents do not know the method of cervical cancer screening. The majority of the respondents (56.0%) obtained information on cervical cancer screening from the mass media.
For the study of Phuong et al. [5], meanwhile, health education and promotion programs for cervical cancer prevention are usually focused on HPV vaccination, educational and promotional materials focused on characteristics and risk factors for the disease i.e. more to women living in rural areas. This may be associated with higher incidence rates of cervical cancer in rural areas.
The study of Woldu et al. [6], showed less than half of the participants were able to mention at least one symptom of cervical cancer. What is more troubling is half of the participants (52%) reported that cervical cancer was incurable even when diagnosed at an early stage. Therefore, the emphasis on health education is very much needed on the symptoms of cervical cancer because it can help women to recognize the disease and get treatment earlier.
But for the study of Rohani et el. [7], meanwhile, it shows that the level of knowledge and awareness of nursing students is high. Race and marital status influence knowledge while gender status and family history of cervical cancer will influence awareness. High knowledge and awareness will impact a positive attitude in undergoing regular cervical cancer screening.
Methodology
Study Location
To collect samples, this study focused on health facilities in Dungun District, Terengganu. Because the problem statement of the study centred on the respondents in Dungun District, Dungun District was chosen as the study location. Dungun District and Kuala Terengganu are 70.06 kilometres apart. This district is managed by the Dungun Town Council (MPD). Apart from that, the Dungun District Health Office in Dungun, Terengganu, has a government hospital, Dungun Hospital, as well as 7 health clinics.
There are two types of health clinics in the United States: urban and rural [8]. Paka Health Clinic (KKP), Kuala Dungun Health Clinic (KKKD), and Kuala Abang Health Clinic are the urban facilities (KKKA). Meanwhile, the Ketengah Jaya Health Clinic (KKKJ), Al-Mutafi Billah Shah Health Clinic (KK AMBS), Bukit Besi Health Clinic (KKBB), and Jerangau Health Clinic are all located in rural areas (KKJ).
Dungun has a total population of 140,741 persons (Basic Population Data of Dungun District from 2016-2019). Women between the ages of 30 and 65 will participate in this case study. In Dungun District, there are 23,969 urban women aged 30 to 65. Meanwhile, there are 12,360 rural women [8]. Figure 1 depicts a map of Dungun District as well as a map of each mukim in Dungun District that houses health facilities. The Dungun District Map and the map of each land sub-district that houses the Dungun District health facility are shown in Figure 1.

Research Design
This is a comparative cross-sectional study. The goal of this study was to compare the knowledge of urban and rural women concerning cervical cancer. A questionnaire will be employed in this investigation as a component. Both urban and rural women will be asked to fill out questionnaires. The data from the samples was then evaluated and statistical significance and tests were reported. The findings of following statistical tests will be used to draw conclusions about the study under consideration. For researchers, this comparative cross-sectional study approach can provide precise and transparent data while also meeting the research question’s needs.
Research Period
This study will run for one year, from 1 December 2020 to 30 November 2021. Data collection using survey forms can be completed within a set time frame with the cooperation of study participants.
Research Population
The study’s target group comprised of women who fit the requirements, particularly those aged 30 to 65 years [9]. According to statistical data on the achievement of pap smear services for health clinics in Dungun District, this study will include women from two categories: urban women and rural women. The study population consists of women aged 30 to 65 who are permanent residents of Dungun District, Terengganu, who visit health clinics in urban (KKP, KKKD, and KKKA) and rural (KKKJ, KK AMBS, KKBB, and KKJ).
Sampling
Sampling Criteria and Sampling Exclusion Criteria
Sampling Criteria: For both urban and rural women, the criteria for eligible women are that pap smear screening is only extended to reproductive women between the ages of 30 and 65 [9]. The third condition is married women [10], which means they have had or are having sexual intercourse. This is due to the fact that the woman is one of the at-risk women who requires pap smear testing.
Exclusion Criteria:The selection of sample exclusion criteria was not given to cervical cancer patients [10], or non-citizens because the primary goal is to identify people at risk for cervical cancer early and provide rapid treatment and follow-up.
Sampling Method
Purposive sampling based on sampling criteria and sample exclusion criteria was employed to select samples for the study. This sample approach was used on anyone in the population who met the requirements and volunteered to participate in the study.
This strategy seeks to both describe the researcher’s problem and provide a representative value in order to meet the study’s objectives. Even sampling was done depending on the clinic’s operational area’s permanent population. Women who visit the clinic in areas other than the operating room will not be sampled. The sample is also separated into two groups: urban women (KKP, KKKD, and KKKA) and rural women (KKP, KKKD, and KKKA) (consisting of KKKJ, KK AMBS, KKBB, KKJ). The study sample will be issued an Index Number (ID) based on the registration number or admission of women in health clinics to discriminate between urban and rural populations. This is addressed in the section on sample size.
Sample Size
To estimate the sample size, several procedures must be completed, including sample size calculations using the formula of two populations based on proportion [11]. The population for determining the sample size was derived from statistical data on pap smear services provided in accordance with the state slide target and the number of slides in 2018 and 2019 at the Dungun District health facility. Table 1 displays the number of slides produced by the Dungun District health facility in 2018 and 2019 in relation to the state’s pap smear target.
Table 1:Achievement of Pap Smear in Health Clinics in Dungun District for 2018 and 2019 based on State Targets.

Step 1: Determine the incidence rate
To determine the incidence rate for women undergoing pap smears in urban and rural areas, researchers used a two -population formula [11], based on the proportions below:

The incidence rate of women who had pap smears in the urban in 2018 and 2019:
The incidence rate of women who had pap smears in the rural in 2018 and 2019:
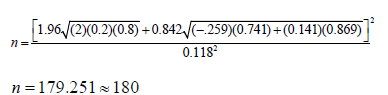
Step 2: Determine the minimum sample size for the two populations
If the sample sizes of the two populations are the same, n1 = n2

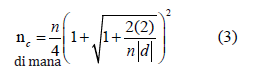
For small sample sizes, continuity correction is used
P1 The proportion of women undergoing pap smears for rural
areas
P2 The proportion of women undergoing pap smears for urban
areas
d = P1 – P2 The difference between the two proportions
Find the following values:
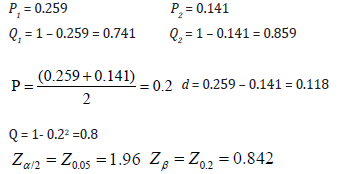
Using a formula (2):
Using continuity correction;
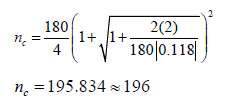
Therefore, if n1 = n2, the minimal sample size for rural is and urban. The total sample size is 196+196 = 392. The sample size for urban women is 196 samples, namely KKKD 66 samples, KKP 65 samples and KKKA 65 samples. While the sample of rural women is also 196 samples where KKBB, KKJ, KKKJ and KK AMBS are 49 samples per clinic. Table 2 shows the sample size to be taken based on the categories of urban and rural women.
Table 2: Sample Sizes Based on Urban and Rural Women Categories.

The sampling method to be used is purposive sampling. Index numbers (IDs) will be assigned to the study sample according to patient admission numbers for urban and rural women in health clinics can be referred to in table 3.
Research Instruments
In this study, the instrument that has been known for sure is a self -administered questionnaire that is related to “Effectiveness of KAP on Cervical Cancer” [12]. This survey question was to assess women’s level of knowledge and attitude towards cervical cancer and pap smear. The entire instrument contains only 56 question items and is divided into Section A, Section B and Section C. Item Part A includes 9 background questions as well as general information such as age, ethnicity, educational level, expected income, marital status, menstruation status, family planning status, and pap smear examination status.
Table 3:IDs of Urban and Rural Women in Health Clinics.

This question is based on a study by [12]. The questionnaire is in Malay. This study was used to assess the level of knowledge and attitudes of women in Amanah Ikhtiar Malaysia (AIM), Kedah, Malaysia where the majority of women in the study are Malay and the sociodemographics are also more or less the same as the population of the study conducted by researchers. So, this survey question is used as the original. This questionnaire has also obtained permission from the original author to be used as an instrument of this study on 15 January 2020 as attached in the appendix (Appendix A).
Validity and Reliability: The purpose of the validity and reliability test was to see the validity and reliability of the survey questions used in this study. As a result of the analysis, it was found that the Cronbach’s alpha value for all items in the questionnaire was 0.753 in the previous study [12]. The Cronbach’s alpha value for cervical cancer knowledge was 0.849, the Cronbach’s alpha value for pap smear knowledge was 0.660. The Cronbach’s alpha value for pap smear attitude is 0.844. Validity and reliability tests are based on alpha values for the items in the questionnaire, and alpha values greater than 0.7 suggest that the questions or items in the questionnaire are valid. As a result, this study is assessed to be of good reliability, requiring no major corrective actions. Questionnaires were chosen from Sa’adiah et al. [12]’s study, which employed a self-administered questionnaire instrument linked to “Effectiveness of KAP on Cervical Cancer” that was designed according to the researchers’ objectives in this study. The questionnaire is written in Malay so that all respondents may understand it. Although some of the questions may be uncomfortable, it is critical for responders to identify cervical cancer risk factors in order to improve their understanding and attitudes about the disease. This is a question that has been raised in earlier research. Participants’ privacy will be protected, and unless needed by law, no names will be associated to the data collection instrument. To preserve anonymity, a numbering system will be employed. To preserve secrecy, questionnaires were sent in envelopes to responders and collected in sealed envelopes. Respondents will have between 20 and 30 minutes to answer the question. Data will likewise be disposed away after the conclusion of the study.
Variable
Variable Measurement: The measurement scale for each variable in the study hypothesis was used to construct the study tool items because the statistical tests that will be used to analyze the data depend on the type of measurement scale. See table 4 shows the variable measurement scale.
Table 4:Variable Measurement Scales.

Ethical Considerations
The Human Research Ethics Committee (JEPeM) at Universiti Sains Malaysia has given their approval to this study (Reference No.: USM/JEPeM/20080440 and attached). The Ministry of Health Malaysia granted approval for this study through the National Medical Research Registry (NMRR) (Reference No.: NMRR-20-1025- 54433 (IIR)), which is also attached. Before the questionnaire was given to the respondents by the NMRR division, a letter of signed consent was also acquired
Data collection
Data collection is systematically related to relevant information to address the research purpose, objectives and research questions. This study uses a structured data collection method. Basically, it uses a questionnaire form as a data collection tool. Only respon dents who have the eligible criteria and agree to participate in the study will be selected for this study. This participation consent form and questionnaire form will be given to the respondents. Data collection was done after obtaining approval from the Human Research Ethics Committee (JEPeM), Universiti Sains Malaysia (USM). Data collection from each clinic for urban and rural areas was done by researchers in stages. The data collection period for each clinic is set for 3 days only, that is on Sunday until Tuesday during working hours.
Data analysis
Data were analysed using Statistical Package for Social Sciences (SPSS) version 20 software (IBM Corp, 2013). Data analysis requires categorizing, classifying, and summarizing data, defining differences between groups and describing them in meaningful terms to elicit answers to research questions to indicate women’s level of knowledge about cervical cancer and level of screening practice [13]. The statistically significant level is P≤0.05. See table 5 which shows the statistical conclusions.
Table 5:Statistical Conclusions.

Results
Descriptive statistical analysis was conducted on the knowledge level (TP) scores that answered the correct answer based on the group of women shown in table 6. The number of women involved in the study was 196 for the urban category and 196 for the rural category. Based on the percentage of correct answers for the above data sample, it was found that rural women (WLB) gave more correct answers than urban women (WB). For the following 11 TP items (B8, B11, B12, B14, B15, B18, B20, B21, B22, B24 and B30), WB gave more correct answers. Even so, the difference between the percentages of correct answers for WB and WLB for items B8, B11, B14, B15, B24 and B30 was very small. This indicates the TP between WB and WLB is good.
Table 6:Level of Knowledge for Each Item for WB and LB.

WB and WLB have over 70% (B2, B3, B4) level of understanding about the signs of cervical cancer. However, they do not understand that high fat food intake, difficulty conceiving, cancer of other reproductive organs and miscarriage are also causative factors of cervical cancer (TP <40% for B6, B11, B12, B14). Women are seen to be more likely to choose modern methods from practicing traditional medicine in treating cervical cancer. Even so, they were less knowledgeable about radiotherapy treatment (TP <50%) in treating cancer compared to chemotherapy and surgery. The high percentage on B19 items with TP exceeding 87% indicates women are aware that pap smear screening can detect cervical cancer from an early stage. But they are less aware, that pap smears can also detect sexually transmitted diseases (TP for B20 <20%). Their understanding of pap smear screening methods and characteristics of at-risk women was also quite good with TP> 60%. Most women know the right time to have a pap smear screening. However, they are less clear with the best time interval for the next pap smear screening (TP B30 <40%).
Discussion
Overall knowledge level scores among urban women (WB) and rural women (WLB) did not show significant differences in the population. Based on the percentage of correct answers for the data sample, it was found that rural women gave more correct answers, namely 19 items of knowledge level compared to urban women with only 11 items of knowledge level. However, the level of knowledge between the two groups is good and still needs improvement.
The results of the study of Ruddies et al. [14], stated lack of knowledge has proven to be one of the major barriers towards cervical cancer screening. In fact none of the participants in Butajira identified HPV as a risk factor for cervical cancer. While HPV -based screening methods have been improved in many countries and are also part of the guidelines for the prevention and control of cervical cancer in Ethiopia. The study of Ruddies et al. [14], also revealed misconceptions about cervical cancer symptoms, risk factors, risk reduction and pap smear screening. Through the study of Reichheld et al. [15], also explained nearly 85% of the 175 women surveyed had low knowledge of cervical cancer and less than 25% knew of symptoms, risk factors, or preventive measures for cervical cancer in five rural areas around Vellore, Tamil. The findings of a study by Drokow et al. [16], also explained that respondents’ knowledge of cervical cancer risk factors is low although in general women are more positive in performing examinations and vaccinations. Therefore, to further encourage women to support preventive measures, knowledge on the effectiveness of treatment needs to be further enhanced to attract women’s readiness to undergo screening.
Another study from Sawicka [17], too, found that women living in rural, Poland areas had less knowledge about cervical cancer than female respondents from urban areas. This is worrying because women know very little about risk factors, early symptoms of cervical cancer, the purpose of screening and the type of initial treatment given. So, there is a need to provide comprehensive education through awareness campaigns on cervical cancer to women in urban and rural areas.
This trend is almost identical in the study of Burhan et al. [18], in Kuantan, Malaysia. This is because almost half of the respondents have low knowledge about cervical cancer and its prevention. Despite having low knowledge, most respondents have a positive attitude to seek treatment if infected with cervical cancer and try to take the measures outlined to prevent the disease.
According to Rodziah et al. [19], stated that education is highly influential and highly significant on the perception of very low pap smear screening in communities in Alor Setar and Sungai Petani. The knowledge a person possesses is also influenced by information. The information provided is a learning process to improve and understand the knowledge gained. This is because knowledge can also influence attitudes in determining health in a better direction for cervical cancer and pap smear tests.
Even according to Argaheni et al. [20], effective interventions need to be done to increase knowledge about cervical cancer that will promote positive attitudes influencing the prevention and ear ly treatment of individuals in general. The results of the study of Wakwoya et al. [21], in rural areas, the Republic of Indonesia found that the knowledge level score of 95% of study participants who received information about cervical cancer from health professionals compared to those who received information from the mass media. In Malaysia in general, various global screening initiatives and approaches are also planned by the government to eradicate cervical cancer through human papillomavirus (HPV) vaccine, cervical screening and cervical cancer treatment [22].
In conclusion, the findings of this study underline that knowledge should be emphasized to increase awareness in reducing the incidence of cervical cancer among urban and rural women.
Conclusion
The impact of measuring this level of knowledge can have a detrimental effect on individuals, communities and nations. Thus, through the results of this study conducted explains that the knowledge about cervical cancer among urban and rural women is good through the percentage of correct answers. However, the results of this study explain that the level of knowledge needs to be further improved to help encourage women to do early screening for early prevention of cervical cancer. So that the percentage of correct answers that can be given by women reaches 100%. The level of knowledge is enhanced through activities or awareness programs related to cervical cancer by involving all agencies including health workers. During the program, the pros and cons of cervical cancer screening, the direct burden of cervical cancer on the family, community, and country should be well discussed. Strengthening this knowledge about cervical cancer is to curb the growing burden of cancer and help prevent or reduce the effects of cancer on oneself, family and society.
Acknowledgment
We greatly appreciate the contributions of the respondents who participated in this study. We would like to thank you for reviewing and editing the manuscript.
Conflict of Interest
There is no conflict of interest for the authors of this paper.
- Yusni M (2019) Pemeriksaan kanser pangkal rahim masih rendah.
- Hall MT, Simms KT, Lew J, Smith MA, Brotherton JML, et al. (2019) The Projected Timeframe Until Cervical Cancer Elimination in Australia: a Modelling Study. Lancet Public Health 4(1): e19-e27.
- Marlow LAV, Waller J, Wardle J (2019) Barriers to Cervical Cancer Screening among ethnic minority women : a qualitative study. J Fam Plann Reprod Health Care 41(4): 248–254.
- Endalew DA, Moti D, Mohammed N, Redi S, Alemu BW (2020) Knowledge and Practice Of Cervical Cancer Screening And Associated Factors Among Reproductive Age Group Women In Districtic Of Gurage Zone, Southern Ethiopia. A Cross-Sectional Study. PLoS One 15(9): e0238869.
- Phuong NTN, Xuan LTT, Huong LT, Toan DTT, Oh JK, et al. (2020) Knowledge of Cervical Cancer and Human Papillomavirus Vaccines Among Child-Bearing Aged Women in Hanoi, Vietnam. Asian Pac J Cancer Prev 21(7): 1951-1957.
- Woldu BF, Lemu LG, Mandaro DE (2020) Comprehensive Knowledge towards Cervical Cancer and Associated Factors Among Women In Durame Town, Southern Ethiopia. Journal of Cancer Epidemiology 2020: 4263439.
- Rohani M, Fatimah A, Roziah A, Noratika J, Nurul S, et al. (2020) Knowledge and Awareness on Human Papillomavirus Vacination Among Final Year nursing and Medical Students in Universiti Kebangsaan Malaysia Medical Centre. Ijmaes 6(4): 899-908.
- Hassadi (2019) History Dungun & Population In Each Mukim: Dungun Land & District Office, Terengganu.
- Roland KB, Benard VB, Greek A, Hawkins NA, Lin L (2016) Changes in Knowledge and Beliefs about Human Papillomavirus and Cervical Cancer Screening Intervals in Low-Income Women After an Educational Intervention. J Pri Care Community Health 7(2): 88-95.
- Hossein Ashtarian E, Mirzabeigi E, Mahmoodi M, Khezeli (2017) Knowledge about Cervical Cancer and Pap Smear and the Factors Influencing the Pap test Screening among Women. Int J Community Based Nurs Midwifery 5(2): 188-195.
- Lemeshow S, Lwanga SK (1991) Sampel Saiz Determination in Health Studies. Wold Health Organization.
- R Romli, S Shahabudin, N Saddki, N Mokhtar (2019) Cervical Cancer and Pap Smear Screening: Knowledge, Attitude and Practice among Working Women in Northern State of Malaysia. Med J Malaysia 74(1): 8-14.
- Kelley K, Clark B, Brown V, Sitzia J (2003) Good Practice in the Conduct and Reporting of Survey Research. Int J Qual Health Care 15(3): 261-266.
- Ruddies F, Gizaw M, Teka B, Thies S, Wienke A, et al. (2020) Cervical Cancer Screening in Rural Ethiopia: A Cross-Sectional Knowledge, Attitude and Practice Study. BMC Cancer 20(1): 563.
- Reichheld A, Mukherjee PK, Rahman SMF, David KV, Pricilla RA (2020) Prevalence of cervical cancer screening and awareness among women in an urban community in South India—a cross sectional study. Ann Glob Health 86(1): 30.
- Drokow EK, Zi L, Han Q, Effah CY, Agboyibor C, Sasu E, et al. (2020) Awareness of Cervical Cancer and Attitude Toward Human Papillomavirus and Its Vaccine Among Ghanaians. Front Oncol 10: 1651.
- Sawicka M (2021) A cross-sectional study to assess knowledge of women about cervical cancer: an urban and rural comparison. Environ Health Prev Med 26(1): 64.
- Burhan M, Rahman N, Haque M (2021) Knowledge and attitude regarding cervical cancer and its prevention among young female adults in Kuantan, Malaysia. J Educ Health Promot 10: 332.
- Rodziah Romli, Sa’adiah Shahabudin, Norkhafizah Saddki, Norehan Mokhtar (2020) Effectiveness Of A Health Education Program To Improve Knowledge And Attitude Towards Cervical Cancer And Pap Smear: A Controlled Community Trial In Malaysia. Asian Pac J Cancer Prev 21(3): 853-859.
- Argaheni NB, Wirakusumah FF, Tobing MDL, Herman H, Sunjaya DK, et al. (2020) Mobile Phone Text Messaging Cross Platform Intervention for Cervical Cancer Screening: Changes In Knowledge And Attitude In Rural Areas Pre- Post Intervention. Jurnal Ners Dan Kebidanan Indonesia 8(2): 123-133.
- Wakwoya EB, Gemechu KS, Dasa TT (2020) Knowledge of Cervical Cancer and Associated Factors Among Women Attending Public Health Facilities In Eastern Ethiopia. Cancer Manag Res 12: 10103-10111.
- Keane A, Ng CW, Simms KT, Nguyen D, Woo YL, et al. (2021) The road to cervical cancer elimination in Malaysia: Evaluation of the impact and cost-effectiveness of human papillomavirus screening with self-collection and digital registry support. Int J Cancer 149(12): 1997-2009.
-

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


